HealthXchange will NEVER ask you to transfer money over a call. If in doubt, call the 24/7 ScamShield helpline at 1799, or visit the ScamShield website at www.scamshield.gov.sg.
Improving the healthcare system | Part 2: Plugging the gaps
25 Aug 2016 | Tomorrow's Medicine
This nine-part series with the SingHealth Office of Strategy Management provides an overview of how the SingHealth Duke-NUS Academic Medical Centre (AMC) is approaching the health challenges facing the nation.
By Professor Terrance Chua Group Chairman Medical Board, SingHealth Medical Director, National Heart Centre Singapore
When I first started practising as a cardiologist in the 1980s, there were only two main treatments recommended for heart attacks. Today, there are numerous recommendations based on multiple studies; and new knowledge is being constantly generated with some 75 clinical trials in cardiology published daily.
Medicine has advanced at a phenomenal rate in the last few decades. At the same time, there is a trade-off: The remendous growth in knowledge has rendered it impossible for a single doctor to know everything about all aspects of medical care. In response, sub-specialisations have proliferated, enabling each doctor to focus on deepening his expertise in one specialty area.
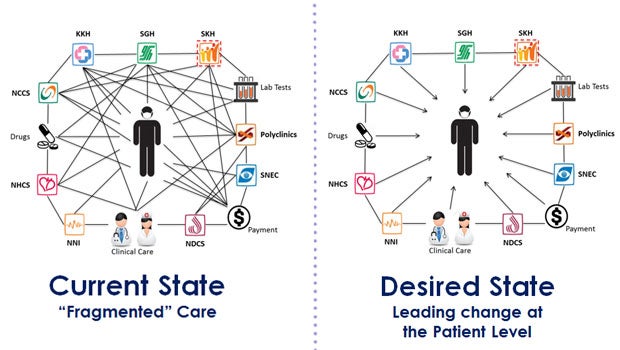
This has started to present challenges for effective care delivery as more patients, especially the elderly, develop increasingly complex health issues. The patient ends up having to see several specialists for the different conditions they have.
This not only causes a great deal of inconvenience and confusion for the patient, but it also adds additional stress to the healthcare system. This system of care is not sustainable.
Instead of proliferating medical sub-specialities, we should create pathways to treat patients with complex conditions in a holistic manner. We have already begun to do that by establishing SingHealth Duke-NUS Disease Centres (SDDCs), which comprise teams of multidisciplinary professionals collaborating to streamline care for specific conditions.
"Instead of proliferating medical sub-specialities, we should create pathways to treat patients with complex conditions in a holistic manner."
How do SDDCs change the way we work? In conventional care, a General Practitioner might refer a patient with a nodule (growth of abnormal tissue) in his neck to a thyroid specialist or surgeon, who would then refer the patient for imaging tests. If the nodule is found to be a cyst, the patient is given an appointment for a biopsy. By this time, the patient would have made at least three trips to the hospital.
At the Head & Neck SDDC, patients can go through the whole process in one visit, saving them time and money and facilitating timely treatment. It also translates to greater work efficiency for clinicians.
This new way of collaborative care emphasises developing a comprehensive database of patients for care and research. In the long term, it will change the way we recommend treatments – as outcomes are collectively measured and studied for improvements in protocols.
There are multiple opportunities to streamline care through cross-institutional collaborations even outside SDDCs. For example, the SGH Department of Emergency Medicine has been working with the National Heart Centre of Singapore (NHCS) to streamline tests for SGH A&E patients with chest pains within 42 to 78 hours of their visit. This omits the need for a separate referral to NHCS and increases access to timely treatment for the patient.
As we modify systems and streamline processes to enhance access to care and increase efficiency, we must do it with the patient in mind. We need to constantly ask the question, ‘How will the patient benefit?’.
The way to approach the increasing complexity and cost of care is to collaborate, not create more silos.














 Get it on Google Play
Get it on Google Play