GPs hold the key to the early identification and treatment of thumb base arthritis, with many cases able to be managed effectively in their care. Singapore General Hospital shares more.
General practitioners hold the key to the early identification and treatment of thumb base arthritis, with many cases able to be managed effectively in their care. Singapore General Hospital shares how to manage in primary care, key considerations for referral to specialist care, as well as the surgical options available.
THUMB BASE ARTHRITIS: A COMMON DEGENERATIVE CONDITION
Thumb arthritis is common with ageing. The most frequent site in the thumb is at the basal joint, also known as the first carpometacarpal joint (CMCJ). Most thumb base arthritis cases result from degenerative (wear and tear) conditions, where friction from the bones rubbing against each other causes the joint cartilage to wear away. It affects up to 10% of the middle-aged female population, with incidence increasing with age.¹
PATHOANATOMY
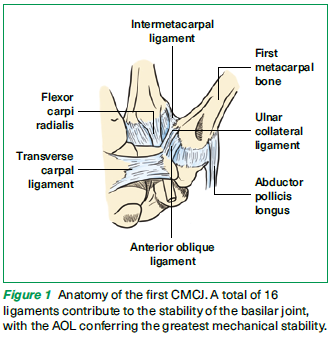
The first CMCJ is a double saddle joint anatomy between the first metacarpal base and trapezium that allows for multiplanar motion, including prehension, opposition and circumduction (Figure 1). Many ligaments surrounding the CMCJ confer stability to the joint, with the primary stabiliser being the deep anterior oblique ligament (AOL).¹
High compressive forces across the CMCJ during pinching can reach up to 12 times the applied load (i.e., 1 kgf of pinch confers 12 kgf at the CMCJ).² This makes the thumb base highly susceptible to early cartilage wear compared to other joints.
PRESENTATION
Thumb base arthritis is more common in women than men and typically occurs after 40 years of age. Prior injuries or fractures increase the risk of developing this condition. Manual workers who engage in frequent tight pinching or gripping activities (such as using screwdrivers or wrenches) are also more susceptible.
SYMPTOMS
Pain and aching at the base of the thumb with pinching and gripping activities (e.g., opening a jar, turning a key or opening a door)
Swelling and tenderness of the thumb base
Crepitus of the thumb base
Deformity and ‘squaring’ appearance of the thumb base
Loss of pinch strength
Limited motion and reduced first webspace span
PHYSICAL EXAMINATION
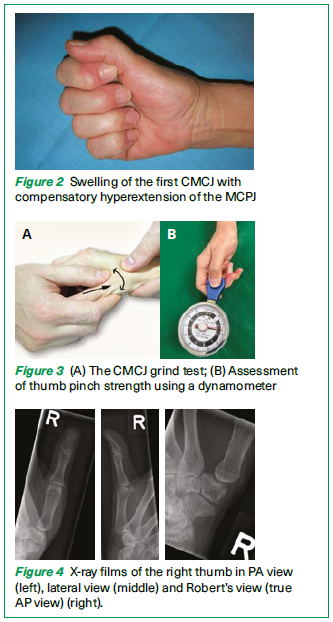
In the early stages, the thumb base may be swollen and tender. Late deformities include subluxation and ‘squaring’ of the CMCJ, hyperextension of the thumb metacarpophalangeal joint (MCPJ), and an adducted thumb with reduced first webspace span (Figure 2).
The provocative CMCJ grind test may reveal pain with crepitus. This is performed by axial loading of the CMCJ and passive ranging of the thumb (Figure 3A). The examiner stabilises the wrist with one hand, and applies axial load and rotatory motion on the thumb axis with another hand. A positive test would produce pain at the CMCJ.
A routine screening of the joint motion by performing circumduction, adduction and abduction, and demonstrating routine activities such as writing and key holding is useful to determine severity.
We often perform the dynamometer pinch test to compare the pinch strength of both sides as an objective measurement (Figure 3B).
The differential diagnosis for thumb base arthritis includes De Quervain’s tenosynovitis, carpal tunnel syndrome and trigger thumb. These conditions may co-exist. In the event of prior trauma, fractures or ligament sprains should be ruled out.
DIAGNOSTIC INVESTIGATIONS
Radiographic imaging
Basic radiographs include a thumb X-ray with standard posteroanterior (PA) and lateral views. Special views to evaluate the joint include Robert’s view, which offers a true AP view with adequate exposure of the peritrapezial joint (Figure 4).
The X-ray may reveal narrowing of the joint space, subchondral cyst formation and bone spur formation. In severe stages, subluxation of the joint and involvement of the adjacent scaphotrapezotrapezial (STT) joint may be seen.
Classification of radiographic progression
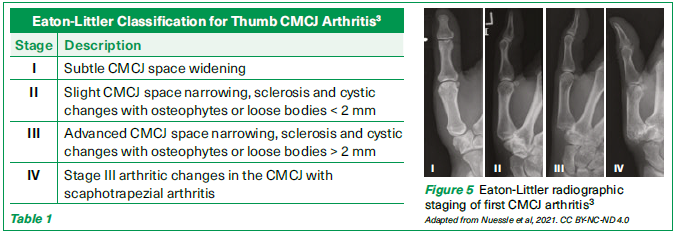
The Eaton-Littler classification is widely used to describe the four stages of radiographic progression in CMCJ arthritis (Table 1 & Figure 5). However, this classification demonstrates moderate to weak reliability and correlates poorly with symptom severity or treatment outcomes.¹
Treatment for Thumb Base Arthritis
1. NON-SURGICAL TREATMENT
Thumb base osteoarthritis has periods of exacerbation and remission. In its early stages, it can respond to non-surgical management. This includes:
Activity modifications
These include to limit, modify and avoid activities that exacerbate symptoms.
Heat therapy
Heat therapy (including warm water immersion, paraffin wax treatment and heating pads) can reduce stiffness, alleviate pain and improve joint mobility in thumb CMCJ arthritis. These methods are simple, effective and can be used daily to enhance joint function and comfort.
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Oral options: Ibuprofen 200-400 mg every 4-6 hours (maximum 1.2 g/day) or Arcoxia (etoricoxib) 60-120 mg once daily for 7-14 days. The dosage should be adjusted based on the patient’s renal function and overall health.
Topical options: NSAID gels or creams can be applied directly to the affected joint to reduce localised pain and inflammation, offering an alternative for patients with contraindications to oral NSAIDs.
Splints
A supportive splint may be used to limit the thumb’s motion and allow the joint to rest (Figure 6). This form of orthosis can be a pre-made ‘Push’ brace or one custom-made by an occupational therapist. The splint should be worn during the day to prevent aggravation or worn at night to rest the joint. Interval exercises strengthen the surrounding stabilising muscles and prevent stiffness from complete immobilisation.⁴
Intra-articular corticosteroid injections
Intra-articular corticosteroid injections may temporarily relieve and improve function for patients whose symptoms do not respond to conservative measures. The effects typically last for 3 to 6 months.5

2. SURGICAL TREATMENT
If the patient has persistent pain and functional impairment, multiple surgical options are available. The nature of surgery is highly dependent on patient factors such as age and functional demand, as well as the stage of disease.
Techniques for CMCJ reconstruction vary based on the symptoms and severity of osteoarthritis. There are two main broad categories – joint preserving and non joint preserving (Table 2).
Joint preserving
| Non joint preserving
|
1. CMCJ arthroscopy 2. Metacarpal osteotomy 3. Total joint replacement (implant arthroplasty)
| 1. Trapeziectomy with or without ligament reconstruction tendon interposition (LRTI)
2. Trapeziectomy with suspensionplasty
3. CMCJ fusion
|
JOINT PRESERVING
1. CMCJ arthroscopy
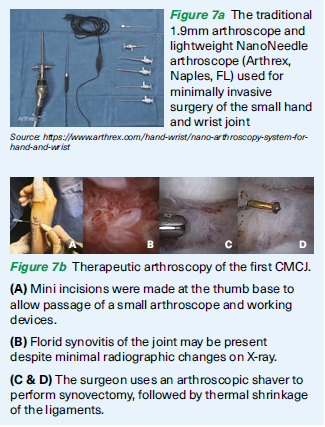
This is a minimally invasive procedure offered to patients with early-stage, symptomatic arthritis. Typically, the traditional 1.9mm arthroscope or a modern NanoNeedle scope is used for small joint surgery of the hand and wrist (Figure 7a).
The surgeon creates a mini incision at the base of the thumb and uses a small camera (arthroscope) to evaluate the joint cartilage, perform synovitis and stabilise ligaments through thermal shrinkage (Figure 7b).
This technique preserves the joint’s normal anatomy, and current evidence suggests that it provides therapeutic benefits including longterm pain relief and improved joint stability6.
This procedure can be performed alongside a partial trapeziectomy (removal of part of the trapezium) and suspensionplasty, which helps support the first metacarpal and prevents it from sinking, reducing the risk of metacarpal-scaphoid arthritis.
2. Metacarpal osteotomy
This can be considered for early-stage symptomatic cases. The procedure involves creating a precise cut through the metacarpal bone and stabilising it with metal plates. The aim is to redistribute the mechanical load across the joint while preserving the articular surfaces.
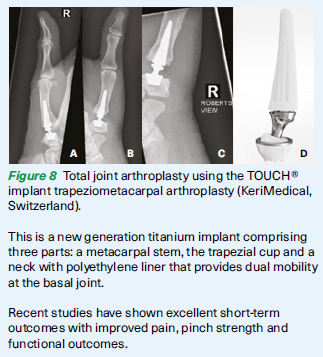
3. Total joint replacement (implant arthroplasty)
Total joint arthroplasty of the thumb CMCJ is typically reserved for older patients with lower functional demands, focusing on pain relief and maintaining basic hand function.
First described in 1979,7 this procedure involves replacing the damaged joint surfaces with an implant, similar to a total hip replacement. The development of newer dual mobility implants over the past decade offers improved joint stability, a wider range of motion and a lower complication rate (Figure 8).8
Potential complications include implant loosening, joint subluxation and fractures of the trapezium bone.9
A recent study demonstrated superior early recovery, key pinch strength and earlier return to work between CMCJ arthroplasty and the traditional trapeziectomy with suspensionplasty.10
NON JOINT PRESERVING
1. Trapeziectomy with or without ligament reconstruction tendon interposition (LRTI)11
This is commonly recommended for advanced osteoarthritis (stage III/IV) with bony changes.12 This technique involves excising the trapezium bone and rerouting the native tendon (usually the flexor carpi radialis tendon) to stabilise the weakened thumb ligament.
The goal is to achieve anatomic reconstruction of the ligaments to preserve thumb base biomechanics.13
Some surgeons may choose to remove part or all of the trapezium, with or without ligamentoplasty, as current evidence shows no clear advantage of one procedure over the other.14
2. Trapeziectomy with suspensionplasty
This procedure is less commonly performed. The technique supplements the traditional trapeziectomy by using a strong suture device to create suspension between the first and second metacarpal bones, preventing the subsidence of the first metacarpal bone following trapezium excision. Suspension can also be achieved using an internal brace suture tape or a mini tightrope.
3. CMCJ fusion
Joint fusion (also known as arthrodesis) between the metacarpal base and trapezium may be offered to younger patients and labourers with high functional demands. This procedure involves the fusion of the first metacarpal bone to the trapezium bone, providing superior stability and grip strength1, helping to offload the basal joint.
Patients should be informed that while they will permanently lose joint mobility following surgery, they can expect significant pain relief.
WHEN TO REFER TO A SPECIALIST
General practitioners (GPs) play a vital role in the early identification and management of thumb CMCJ arthritis. While many cases can be managed conservatively, certain scenarios warrant referral to a hand surgeon for specialised care.
Below are key situations when referral should be considered.
Criteria
| Details
|
Persistent symptoms despite conservative treatment
| Pain, swelling or functional limitations that do not improve with rest, splinting, NSAIDs or heat therapy
|
Progressive deformities
| Visible subluxation, squaring of the thumb base or hyperextension at the thumb MCPJ
|
Severe functional impairment
| Difficulty performing daily tasks, such as gripping, pinching or writing, that affects the patient’s quality of life
|
Suspected advanced disease
| Clinical signs of advanced arthritis (e.g., joint instability or significant reduction in thumb mobility), particularly with radiographic evidence of stage III/IV arthritis
|
Criteria
| Details
|
Younger patients with high functional demands
| Patients who are manual labourers or require fine motor skills for their occupation and may benefit from joint-preserving procedures
|
Failure of corticosteroid injections
| When intra-articular corticosteroid injections provide only short-term relief or fail to alleviate symptoms entirely
|
Prior trauma or injury
| History of thumb fractures, ligament injuries or untreated dislocations requiring evaluation for secondary arthritis or instability
|
Unclear diagnosis
| Cases with overlapping symptoms of conditions like De Quervain’s tenosynovitis or carpal tunnel syndrome
|
Benefits of referral
Referring patients to a hand surgeon ensures that they receive a comprehensive evaluation and are informed of treatment options tailored to their specific needs. Early referral for surgical interventions, such as arthroscopy, trapeziectomy or arthroplasty, can improve outcomes in patients with progressive or advanced disease.
REFERENCES
Wolfe, Scott W., et al. Green's Operative Hand Surgery. 8th ed., Elsevier, 2022. 2 vols.
Cooney W.P., III, Chao E.Y. Biomechanical analysis of static forces in the thumb during hand function. J Bone Joint Surg Am. 1977;59:27–36.
Eaton RG, Glickel SZ. Trapeziometacarpal osteoarthritis. Staging as a rationale for treatment. Hand Clin. 1987;3(4):455-471.
Neumann DA, Bielefeld T. The carpometacarpal joint of the thumb: stability, deformity, and therapeutic intervention. J Orthop Sports Phys Ther. 2003;33(7):386-399. doi:10.2519/jospt.2003.33.7.386
British Society for Surgery of the Hand Evidence for Surgical Treatment (BEST) Topic: Evidence-Based Management of Thumb Base Osteoarthritis. https://www.bssh.ac.uk/_userfiles/pages/files/Research/Evidence%20based%20management%20of%20adults%20with%20thumb%20base%20osteoarthritis.pdf
Shehovych A, Lawson R, Graham DJ, Sivakumar BS. Outcomes of Arthroscopic Debridement of the First Carpometacarpal Joint: A Systematic Review. J Hand Surg Asian Pac Vol. 2024;29(4):281-285. doi:10.1142/S2424835524500279
de la Caffiniere JY, Aucouturier P. Trapezio-metacarpal arthroplasty by total prosthesis. Hand. 1979;11(1):41-46. doi:10.1016/s0072-968x(79)80007-8
Herren DB, Marks M, Neumeister S, Schindele S. Low complication rate and high implant survival at 2 years after Touch® trapeziometacarpal joint arthroplasty. J Hand Surg Eur Vol. 2023;48(9):877-883. doi:10.1177/17531934231179581
Holme TJ, Karbowiak M, Clements J, Sharma R, Craik J, Ellahee N. Thumb CMCJ prosthetic total joint replacement: a systematic review. EFORT Open Rev. 2021;6(5):316-330. Published 2021 May 4. doi:10.1302/2058-5241.6.200152
Herren DB, Marks M, Neumeister S, Schindele S. Short-term recovery after implant versus resection arthroplasty in trapeziometacarpal joint osteoarthritis. J Hand Surg Eur Vol. 2023;48(10):1048-1055. doi:10.1177/17531934231188407
Eaton RG, Littler JW. Ligament reconstruction for the painful thumb carpometacarpal joint. J Bone Joint Surg Am. 1973 Dec;55(8):1655-66. PMID: 4804988
Yuan F, Aliu O, Chung KC, Mahmoudi E. Evidence-Based Practice in the Surgical Treatment of Thumb Carpometacarpal Joint Arthritis. J Hand Surg Am. 2017;42(2):104-112.e1. doi:10.1016/j.jhsa.2016.11.029
Shah DS, Middleton C, Gurdezi S, Horwitz MD, Kedgley AE. The effect of surgical treatments for trapeziometacarpal osteoarthritis on wrist biomechanics: a cadaver study. J Hand Surg Am. 2020;45(5):389–398
Wilcke MK, Evans K, Franko MA, Arner M. Trapeziectomy with or without a tendon-based adjunct: a registry-based study of 650 thumbs. J Hand Surg Eur Vol. 2022;47(7):728-733. doi:10.1177/17531934221086220
Dr Nah Jie Hui is a Medical Officer at the Department of Hand & Reconstructive Microsurgery, Singapore General Hospital. She graduated from the National University of Singapore in 2023 and has a special interest in hand surgery. She is passionate about providing patient-centric care and contributing to clinical research.
Dr Abby Choke is an Associate Consultant from the Department of Hand & Reconstructive Microsurgery, Singapore General Hospital. She completed the Singapore Integrated Hand Surgery Residency Programme in August 2024 and was awarded the best performing resident in the exit examination. She has a special interest in complex reconstructive hand surgery and microsurgery.
Dr Chung Sze Ryn is a Singapore and European Board Certified Hand Surgeon from the Department of Hand & Reconstructive Microsurgery at Singapore General Hospital. She specialises in minimally invasive hand/wrist and upper limb spasticity surgery. She graduated from the Royal College of Surgeons, Ireland in 2011 with an MBBCh BAO degree and achieved her MRCS (Edinburgh) and MMed (Surgery) in 2013 and 2016, respectively. She completed her hand residency training in 2020 and was awarded as a Fellow of the Academic of Medicine Singapore (FAMS) in hand surgery. She is currently the Asia Pacific Wrist Association (APWA) fellowship chairman in minimally invasive wrist surgery.
GP Appointment Hotline: 6326 6060
GPs can scan the QR code or visit the website more information about the department.
